Menu
Contents:
Menu
- ICD deactivation
- Decision aids
- Applying donut magnet
Ethical and Legal considerations when considering ICD deactivation:
The decision to switch off an ICD must be a shared decision, with full involvement of the person and their loved ones, as well as the healthcare team caring for them. It must be based on a careful assessment of the person’s individual circumstances. When a person lacks capacity, the decision must be made in their best interests as per the Mental Capacity Act (Department for Health, 2005). The views of those close to the person must be considered when making a best-interests decision.
Ideally, the initial discussion around when it would be appropriate to switch off an ICD should be at the time of insertion of the device. This should be revisited at any appropriate appointment such as device checks or day hospice appointments. A change in the patient’s clinical condition should also trigger to re-visit the discussion around ICD de-activation.
Practical considerations:
Planned ICD deactivation:
This should be the aim for the majority of people who require ICD deactivation. This is performed via the cardiac physiologist either in an outpatient clinic setting, at a person’s home, or other setting such as a hospice. It is a non-invasive, and painless procedure, which takes a few minutes. It is important that the person and their family understand that the deactivation of the shock function will not cause their immediate death, but that their ICD will no longer deliver shocks to treat an arrhythmia which could cause their death.
Emergency ICD deactivation:
Occasionally, situations may arise where someone is in their last days of life, either due to a sudden event or where the discussion of deactivation has not occurred in advance. In these situations, if a cardiac physiologist is not available, the ICD can be deactivated by taping a ring (donut) magnet securely to the skin overlying the device. Devices from Biotronik will be inhibited by a magnet for only 8 hours. Therefore, with a Biotronik device (or if manufacturer of device unknown) the magnet must be removed for a few seconds and reapplied every 7 and half hours. Arrangements should be made as soon as is practical for definitive deactivation.
Key Points to explain to people about ICD Deactivation:
- Near the end of your life, your ICD may deliver shocks that are painful and distressing, and will be of no benefit
- It is best to think and decide about deactivation in advance rather than in a crisis
- Deactivation will not cause death
- Once your ICD has been deactivated, if your heart has a rhythm change that can cause death, your ICD will not deliver treatment for it
- Deactivating the shock function does not deactivate its pacemaker function
- Deactivation is painless
- If your condition unexpectedly improves or you change your mind, the ICD can be reactivated
Practical guide
Discussions to deactivate an ICD should be a routine part of advance care planning and should be included in the discussions about DNACPR. Outcomes of discussions should be recorded on the patient’s ReSPECT form (or locally used ACP document). It must be clearly highlighted if the ICD has been deactivated or not.
It is helpful to establish local plans to highlight patients who may be approaching end of life and ensure early discussions and decisions about deactivation of the ICD.
LOCAL CONTACT DETAILS
ICD clinic opening times/contact number/Fax number:
Consultant Cardiologist via switchboard:
Cardiology physiologist:
On call cardiology physiologist:
On call palliative care team:
Patients should have equal access to deactivation facilities regardless of their current place of care and ideally the decision to deactivate should take place when a patient has mental capacity.
This will involve discussions on deactivation with the patient and the people who care for them. The heart failure team or palliative care team may be well placed to do this if they know the patient well.
Speed of deactivation will depend on urgency of need for specific guidance on this see Deactivation of implantable cardioverter-defibrillators towards the end of life A guide for healthcare professionals from the Resuscitation Council UK the British Cardiovascular Society and the National Council for Palliative Care.
The decision to deactivate should involve the MDT which can include medical team looking after them (primary and/or secondary care), the heart failure multidisciplinary team and the palliative care team may also be involved.
Once the decision is made these needs to be recorded in the patient’s notes/system and a deactivation form is completed, this should accompany the patient to the ICD clinic at the time of deactivation.
Details of contacts for support should be documents both in and out of hours so that it is clear who to contact for support.
Any decisions regarding ICD deactivation should be recorded in the patient’s electronic or paper notes. It must be communicated to all other healthcare professionals involved in the person’s care. When a patient consents to deactivation, written consent must be documented. The ICD deactivation consent form in Appendix 1 can be used to do this or the local team may have their own form
When referring for deactivation you can use form in Appendix 2 to help the cardiac physiologists prioritise as an urgent referral.
Decision aid for deactivation of ICD – Routine cases
Clinicians (community nurses, GPs, cardiologists, palliative care team) highlight patient approaching end of life
Complete consent form for deactivation (Appendix 1) & arrange appointment in ICD deactivation clinic
Patient can
go to clinic
Book appointment in deactivation clinic – the patient should be given information about the process of deactivation prior to this appointment & take their completed consent form with them
Following deactivation, a record should be made in the patient’s notes & on their ReSPECT form
Patient can NOT
go to clinic
Contact local cardiac physiology team to arrange a home visit for deactivation– the patient should be given information about the process of deactivation prior to this & have their completed consent form available
Following deactivation, a record should be made in the patient’s notes & on their ReSPECT form
Decision aid for deactivation of ICD – Routine cases
Patient is dying with active ICD in-situ
Utilise donut magnet to prevent shocks being delivered to the patient – magnet can be loaned from local palliative care team/hospice, ICD clinic or on-call cardiology team
If time allows or during working hours contact local cardiac physiology team to arrange deactivation
How to apply a donut magnet
- Ensure the patient is aware why you are placing the magnet and verbal consent is given and consent form is signed if possible.
- Ask the patient to feel and point to where the ICD is located (if possible), if not then look for the scar usually located to the left below clavicle. Alternative placement could be on the right or down under the Left arm around 6th rib.
- Feel for the ICD which will be a solid lump under the skin
- Place the magnet over the lump – you may hear a quiet alarm as the magnet disables therapies.
- Secure the magnet in place with micropore/transpore, as pictured, to ensure the magnet does not move.
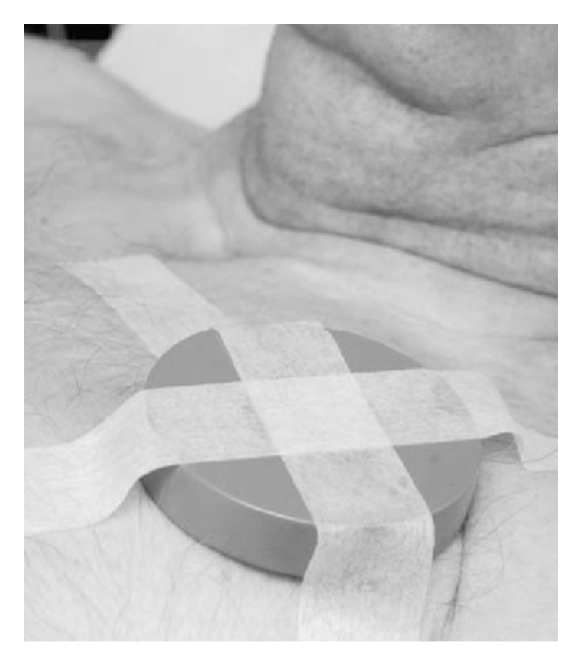
PLEASE NOTE IF THE MAGNET IS APPLIED FOR OVER 8 HOURS, YOU MUST REMOVE AND REAPPLY
Please note the following:
- Donut magnet temporarily stops the ICD delivering shock therapies but only whilst in position over the ICD.
- Normal function is restored as soon as it is removed.
- Applying magnet does NOT cause death, it just stops shocks occurring if the patient has an arrhythmia. This stops the ICD delivering any shock or ATP therapy but does not disable bradycardia pacing delivery.
- This is a temporary solution as the ICD will return to normal function as soon as the magnet is removed.
- The ICD will still require deactivation by a cardiac physiologist using a programmer as soon as is practicable.
- This deactivation method may be considered if a planned ICD deactivation was not arranged and a cardiac physiologist cannot get to a patient in time.
Device management after death
Pacemakers (PPM):
In general, PPM do not require any immediate action when a patien dies however it must be highlighted on the cremation form (if applicable) so that it can be safely removed due to the risk of lithium battery explosion.
If a patient dies unexpectedly a cardiac physiologist should undertake early interrogation of the device to determine heart & device rhythm behaviour immediately before death. This information may be useful to the coroner
ICDs/CRTDs:
A magnet should remain in place over the device after death until a cardiac physiologist can deactivate the ICD. Removal of the device should not be attempted until it has been deactivated as there is a risk that the operator may receive a shock.
As above, if the death is unexpected, the device should be interrogated by a cardiac physiologist at the earliest opportunity.
Disclaimer (SPAGG - Rewrite)
This Guide is intended for use by healthcare professionals and the expectation is that they will use clinical judgement, medical, and nursing knowledge in applying the general principles and recommendations contained within. They are not meant to replace the many available texts on the subject of palliative care.
Some of the management strategies describe the use of drugs outside their licensed indications. They are, however, established and accepted good practice. Please refer to the current BNF for further guidance.
While WMPCPS takes every care to compile accurate information , we cannot guarantee its correctness and completeness and it is subject to change. We do not accept responsibility for any loss, damage or expense resulting from the use of this information.